Much uncertainty exists about thelasting impact the COVID-19 pandemic will have on our personal and professional lives. In the hearing care professions, there will be anincreased focus on the need to sanitize items that come in frequent contact with patients, such as transducer cables from audiometers, immittance instruments, OAE analyzers, and hearing instrument verification systems, just to name a few. It’s also quite possible that, at least for the near future, hearing care professionals (HCPs) will want to limit close contact with patients. In a profession that requires close contact during almost all patient encounters, this is going to be a challenge, to say the least.
One service many HCPs provide to their patients is hearing instrument verification byperforming real ear measurement using speech mapping. The use of real ear measurement for fitting hearing aids to adult patients is considered a best practice by both the American Academy of Audiology and American Speech-Language Hearing Association (1). According to Mueller, “there is not suitable alternative to probe-mic measures when it comes to fitting hearing aids”. (2)
Emphasis on the value of HI verification using real ear measurementand best practice recommendations as well as demand for this procedure from patients, has contributed to an increase in the percentage of HCPs using real ear measurements (personal observation). Nonetheless, the majority of HCPs still do not routinely perform real ear measurement on adult patients.
As recently as 2017, it was estimated that 70%-80% of HCPs do not perform real ear measurement on a regular basis (3).The literature documents improved performance on speech-in-noise tests, user satisfaction, and fewer office visits when real ear measurements are part of the fitting process. It certainly isn’t due to the lack of quality HI verification systems. The systems available today are designed to provide fast, accurate on-ear verification measurements, many integrating with HI manufacturers’ software to provide automatic adjustment of HI gain and output.But, unfortunately, not without havingclose contact with the patient.
So how can anHCP limit close, physical contact with a patient without sacrificing accuracy?One proven method is by using coupler-based verification. This may be more commonly known as “simulated real ear measurement” or S-REM. Regardless of the terminology used to describe the procedure, the goal is to program the HI to match a provider-selected prescriptive fitting target (e.g. NAL-NL2 or DSL 5.0)when connected to an appropriate test coupler or real ear adapter.
Levels measured in the test box are converted to estimated ear canal levels using the RECD values. Additional correction factors for the microphone location effect (MLE) based on the instrument type selected(BTE, RITE, ITE, ITC, etc.) are used to predict the on-ear response. The resultant coupler measured audibility curves should be very close to audibility curves obtained by performing on-ear verification.

Coupler-based programming of hearing instruments is standard practice to verify adequate audibility when fitting a pediatric patient. Since it is challenging to perform on-ear real ear measurementson babies and young children, coupler-based verification is an excellent alternative. (4)There is no reason why this same procedure cannot be successfully applied to adult patients, as well. In fact, many HCPs now utilize coupler-based measurements to predict on-ear performance for their adult patients. Thekey point is the patient does not need to be presentto perform this procedure.
What's Needed? RECD Measurement Options
Hearing aid test/verification systems available from your local e3 office are all capable of coupler-based verification measurements. The measurements can be conducted in a test box or in cases where a test box is not available,by usinga real ear coupler adapter kit. The latter method uses the free field speaker of the probe microphone system to deliver the test stimulus to the hearing aid. The hearing aid is placed on a small base at a distance of 0.5 to 1m from the speaker.
Whether the measurement is done in a test box or outside of a test box using the manufacturer supplied real ear adapter, appropriate correction factors are applied to the coupler measurement (RECD and MLE) to predict how the instrument will perform when measured with a probe microphone in the patient’s ear.
Current users who have a probe mic only system can purchase a real ear adapter kit or a test box from your local e3 office.





What's Involved?
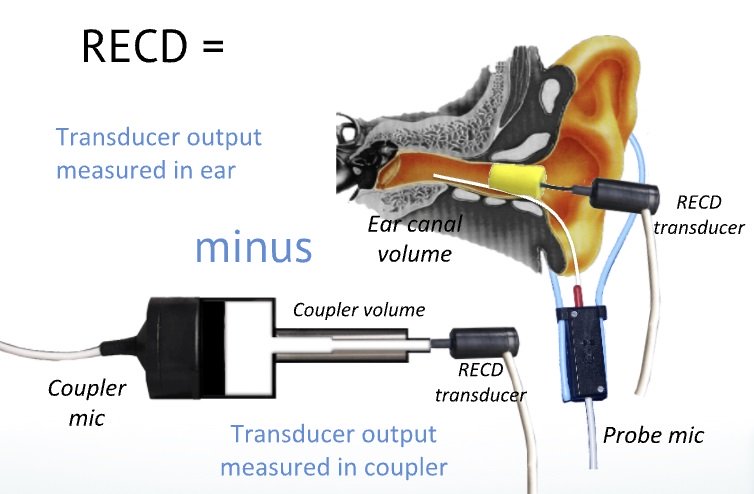
The key to successfully predicting on-ear performancevia coupler measurements is by using a custom real ear-to-coupler difference (RECD) curve. As the name implies, this custom curve accounts for the difference in decibel levels across frequencies between the dB SPL measured in a HA-1 2cc test coupler and the dB SPL in the patient’s ear using the same coupling method, sound source and signal(Fig 3). By taking the short amount of time to make this custom measurement, a more accurate, predicated on-ear curve will be the result. (Please review ANSI S3.46 2016 Methods of Measurement of Real-Ear Performance Characteristics of Hearing Aids for new information about custom RECD measurement).

To appreciate the value of the RECD and the impact it can have on overall accuracy of the fitting, it is important to know the two waysit is utilized in HI verification systems. These are:
- To convert dB HL audiometric thresholds obtained with insert phones to a dB SPL audiogram. These dB SPL thresholds are used to calculate the targets for the prescriptive method selected (e.g. NAL-NL2; DSL 5.0)
dBHL thresholds + ANSI insert phone calibration value + average or custom RECD = dB SPL threshold
- To convert coupler audibility measured levels (in dB SPL)to on-ear audibility predicted levels (also in dB SPL)
Coupler SPL + average or custom RECD + MLE = predicted real ear SPL(5)
How is a custom RECD compared to an age based average RECD going to improve the accuracy of my HI fittings? An average RECD does not take into accounthow the individual differences in ear canal acousticsand impedanceaffect the dB SPL measured at the tympanic membrane (TM). Research has shown that dB SPL measured at the eardrum may vary greatly across listeners with the same dB HL audiogram.(6)Why is that? To answer that question, you have to understand how an audiometer is calibrated?
The air conduction transducers of an audiometer are calibrated in a hard-walled test coupler representing an “average” adult ear canal. For insert earphones, the volume of the test coupler is 2 cc. Most human ear canals have a volume less than 2cc. Therefore, the overall dB SPL in a patient’s ear canal will be higher than that of the 2cc test coupler used to calibrate the audiometer. Since ear canal acoustics are specific to an individual, as previously stated,it’s very likely that patients with the same dB HL audiogram may show extremely variable dB SPL levels when measured at the TM. Correcting for individual ear canal acoustics overcomes the limitations of using an average RECD by accounting for the impact individual ear canal acoustics has on HL to SPL conversion. Not taking the RECD into account can lead to over amplification in most cases and under-amplification in some.
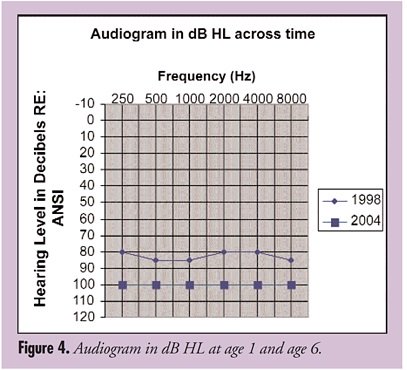
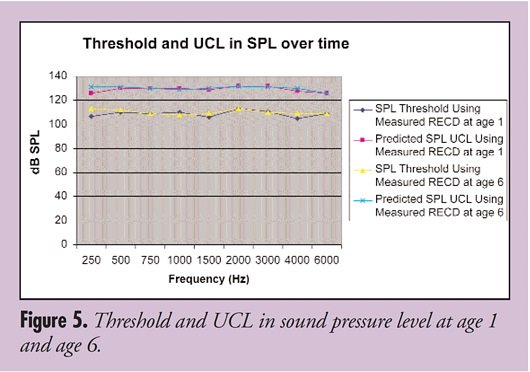
To demonstrate the importance of a measured RECD when converting HL thresholds to SPL, please review the following examplepresented by Palmer (2005) in The Hearing Journal Page Ten column. Figure 4 shows two HL audiograms measured on the same patient at ages 1 and 6 years. It appears that hearing thresholds have gotten worse over the course of five years. Actually, the patient’s hearing did not change, but the size of the patient’s ear canal did; it had become more adult-like. As a result, a higher HL dial setting was required to obtain the same SPL at the TM at age 6 compared to age 1. But when you transform the HL thresholds to SPL, the applied custom RECD revealed that the SPL at the TM had not changed (Fig 5) (8)
Outside of the pediatric population, most HCPs fitting adult patients do not regularly measure a custom RECDsince on-ear verification of audibility is the norm. Nonetheless, there are those who tout the use of coupler audibility verification as a “pre-fitting” tool followed by on-ear confirmation of the coupler measurement at the time the HI is delivered to the patient. Less time is then spent trying to match targetswith the patient present, since the coupler measurement should have accurately predicted the on-ear levels.
I am often asked if it is necessary to measure a custom RECD, particularly if on-ear measurements are the preferred method of verification. Of course, the answer is “no” it is not necessary to measure the RECD, but to ensure a fitting that is as accurate as possible, it is recommended, even in cases when coupler-based measurements are not the norm.
One Other Very Important Point...
Neither the average nor custom RECD is applied to HL to SPL conversion if supra-aural or circumaural headphones are used to obtain pure tone HL thresholds. And, of course, if on-ear measurement is the verification method of choice, again, neither the average nor custom RECD is used.
Are There Limitations?
Unfortunately, the answer is yes, there are limitations to the use of coupler audibility verification to predict on ear performance.
The measurement of a custom RECD assumes thatit completedin a sealed coupler and ear canal; in other words, no venting. According to Bagato and Moodie (2008) (5), any vent larger than 1 mm will affect the accuracy of the predicted on-ear values in the low frequencies (250Hz – 500Hz). When performing coupler-based measurements, the vent is plugged and not accounted for, therefore, some error will be introduced into the conversion to predicted on-ear values. As the vent grows larger or it is a true open fitting, the errors will be greater when using coupler-based verification to predict on-ear levels.
What about RITE or RIC style hearing aids? Almost 80% of the hearing instruments sold in the US in 2019 were RIC. (9) Depending upon the coupling method used, the same limitations apply to RIC fittings, that being, the impact of venting will not be accounted for in the coupler-based measurement. Again, this should only be a problem when matching targets in the frequency range below 1KHz, although in open fits, inaccuracies may extend out to 1.5KHz (10)
The hope is to develop correction factors to account for venting, but as of this writing and to my knowledge, there are none available.
Nonetheless, coupler-based HI verification allows the HCP the opportunity to limit close patient contact, and in combination with a custom RECD, provide a more accurate fitting compared to relying on average values used in first fit algorithms.
To summarize, due to individual differences in ear canal acoustics, a custom RECD improves the accuracy of the SPL thresholds (when using insert phones for audiometry) used to calculate target estimation through the use of prescriptive methods such as NAL-NL2 and DSL. And it is essential if coupler audibility verification is to be used to predict on-ear performance.
Your local e3 representative stands ready to assist in finding ways to effectively respond to new demands due to COVID-19. Please contact your local e3 office for information on coupler-based verification.
Please use the references below and the many other available for more details on the use of custom RECD in your hearing aid fittings.
References
-
Valente, M., Abrams, H., et al (2006). Guidelines for the Audiologic Management of Adult Hearing Impairment. American Academy of Audiology. Retrieved from www.audiology.org
-
Mueller, H.G. (2014, January). 20Q: Real-ear probe-microphone measures - 30 years of progress? AudiologyOnline, Article 12410. Retrieved from: http://www.audiologyonline.com
-
Beck DL. Best practices in hearing aid dispensing: An interview with Michael Valente, PhD. Hearing Review. 2017;24(12):39-41.
-
McCreery, Ryan PhD Building Blocks: RECD Is a Reasonable Alternative to Real-Ear Verification, The Hearing Journal: July 2013 - Volume 66 - Issue 7 - p 13-14 doi: 10.1097/01.HJ.0000432411.23573.80
-
Bagatto, M., Moodie, S (2008 July). Vent Considerations in a RECD with a Vented Earmold. AudiologyOnline, Retrieved from Audiology Online, https://www.audiologyonline.com/ask-the-experts/vent-considerations-in-recd-with-258
-
Audioscan Verification Fundamentals Chapter 3.1 RECD Fundamental www. Audioscan.com
-
Glista, D., Hawkins, M., Moodie, S., Scollie, S. Clinical Changes to RECD Measures: Understanding How the RECD Fits Into the “Big Picture” of Hearing Aid Fitting. Canadian Audiologist, February 2015, 2 (6). Retrieved from https://canadianaudiologist.ca/issue/volume-2-issue-6-2015/column/science-matters/
-
Palmer, C.In fitting kids with hearing aids,ensuring safety and audibility is a good way to start. The Hearing Journal, February 2005, 58 (2): 10-16
-
Powers TA, Rogin CM, MarkeTrak 10: Hearing aids in an era of disruption and DTC/OTC devices. Hearing Review. 2019;26(8):12-20.
-
Personal communication. Chris Stokes-Reese. Audioscan, a division of Etymonic Design, Inc.